Ending Pandemics: US Foreign Policy to Mitigate Today's Major Killers, Tomorrow's Outbreaks, and the Health Impacts of Climate Change
Every U.S. President in recent decades has had to respond to at least one pandemic disease. Political leadership has proven decisive. In the coming years, U.S. foreign policy will face at least three inter-related issues: today’s major pandemics of AIDS, TB, and Malaria; future outbreaks with the potential to become pandemics; and rising risk from infectious diseases associated with climate change. A review of epidemiologic data shows global progress on each issue is threatened. A coordinated U.S. effort, across agencies and engaged with national and multilateral partners, could save lives and address significant foreign policy interests. Such an effort could boost economic prosperity by reducing disease-related lost productivity, which we estimate at $1.7 trillion, with returns to investment in pandemic-related global health efforts averaging 17–20 to 1. Foreign policy focus on pandemics could also address gender and social inequalities and support climate adaptation and mitigation. Pandemic-related global health spending is 0.19% of the U.S. budget—a figure that has been flat in recent years even with growing needs and significant potential gains from investment.

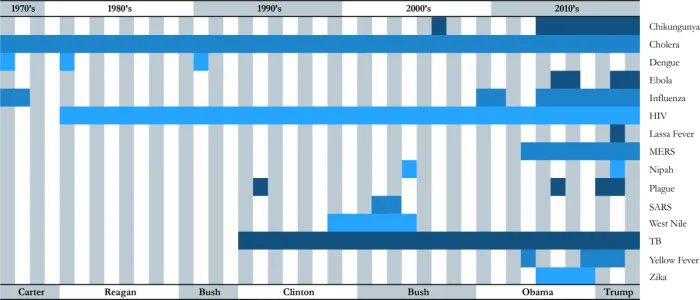
Each U.S. President since Jimmy Carter has had to respond to an international outbreak of infectious disease—often multiple (figure 1). While pandemics are biological phenomena, they are highly amenable to political action—through attention, policymaking, and resource allocation. President Reagan’s inaction contributed to the growth of the global AIDS pandemic, while President George W. Bush’s engagement helped stem its upward trajectory.1 President Obama’s intervention on Ebola, albeit belated, helped galvanize coordinated international action to bring the epidemic under control.2
Today, from AIDS to Ebola to mosquito-borne diseases, political action is insufficient. The struggle to respond to the current Ebola outbreak in the Democratic Republic of Congo, the second most lethal in history, illustrates the challenge.3 Meanwhile, climate change and mass migration are compounding the complexity of the task. How, then, should U.S. foreign policy respond in a world of competing priorities?
This article describes the potential for expanded U.S. foreign policy leadership on pandemics. Saving lives is a worthy goal in itself. The wellbeing of Americans is also inextricably connected with that of people around the world. The oft-repeated reality that diseases know no borders reveals why an approach rooted in international solidarity and multilateralism is needed. We propose a focus on three synergistic areas related to pandemics:
- halting today’s biggest pandemics,
- keeping tomorrow’s outbreaks from becoming pandemics, and
- reducing the rising threat of infectious diseases associated with climate change.
We focus here on pandemics—epidemics of infectious disease affecting a wide geographic area and large numbers of people, and crossing international borders.4 This focus is not intended to direct attention away from other global health priorities, but to identify particular opportunities where U.S. political action could be most impactful, and catalytic for international cooperation, given the U.S. geopolitical position and historical investments in infectious disease programs.
In addition, infectious diseases drive global inequality. Despite increasing mortality from non-communicable diseases, people living in poverty continue to die in large numbers from infectious diseases.5 The effects of pandemics are disproportionately experienced by the poor and marginalized—globally and within countries.6 Young women in sub-Saharan Africa, gay and bisexual men, and transgender people, for example, still face high burdens from HIV.7 During the West Africa Ebola epidemic, the disease and economic impact fell hardest on poor communities.8 Climate change promises to exacerbate adverse effects on marginalized communities.
U.S. administrations in the coming years will have little choice but to address these areas. Progress against AIDS, tuberculosis (TB), and malaria is stalling. Experts agree it is not a question of if, but when, the next major pandemic will occur.9 The frequency and diversity of new outbreaks is growing, with 7,000 signals of potential outbreaks each month, according to the World Health Organization (WHO).10 Without additional action, climate change is poised to put nearly a billion people newly at risk of mosquito-borne viruses.11 Drug-resistant infections are on the rise.12 Yet there remain major gaps in response and preparedness.
The focus here is on U.S. foreign policy—an area where presidents have the strongest prerogative, even as power is shared with Congress.13 We describe significant returns to an expanded foreign policy effort, at a presidential level, on pandemics—both in lives saved and improved global economic prosperity. We note, however, that efforts by the U.S. government can only be effective as part of globally-coordinated, multilateral efforts—which are threatened in the current era of isolationism and populism.14
The article begins with a brief review of the current context of today’s largest pandemics, emerging and re-emerging diseases, and climate-sensitive outbreaks— with brief discussions on opportunities for U.S. action on each. The global economic impact in lost productivity due to infectious disease is then calculated for low- and middle-income countries (LMICs), including fast growing economies and key U.S. trading partners. We also describe estimates of economic return to U.S. investments, which are quite high.15 We then map U.S. global health spending in recent years on these areas, which totals 0.19% of the federal budget, and close with suggestions about key opportunities for structuring a coordinated U.S. pandemics initiative. Together, there is strong evidence that U.S. leadership could help reduce the pandemics that kill millions today, while preventing tomorrow’s outbreaks from becoming global health emergencies and reducing the magnitude and pattern of climate change-related risks.
Halting Today’s Pandemics: HIV, TB, Malaria
After a decade of progress, the response to the world’s leading infectious killers— AIDS, TB, and malaria—is faltering. The diseases killed nearly 3 million people last year.16 Stalled progress is driving inequality as these diseases disproportionately affect marginalized populations including people living in poverty, young women, gay men, children, people who use drugs, and others.17
The U.S. has made political and financial investments in multilateral institutions like the Global Fund to Fight AIDS, TB, and Malaria and in bilateral programs including the President’s Emergency Plan for AIDS Relief (PEPFAR), the President’s Malaria Initiative (PMI), and USAID TB programs (figure 7).
These have augmented domestic financing to achieve results once considered impossible. 23 million people are on HIV treatment; mortality and new infections have been cut in half.18 An estimated 54 million lives have been saved from TB since 2000 and malaria cases reduced by 20 million.19 HIV programs have provided critical human rights resources and the only LGBT-friendly healthcare in many settings. Some countries have achieved remarkable results, like Botswana where 77% of all HIV-positive adults know their status and have attained viral suppression, which has been shown to stop HIV transmission.20 Signs of success on TB and Malaria have also given rise to viable strategies, agreed to by countries at the UN, to end these pandemics as public health threats in the coming two decades.21
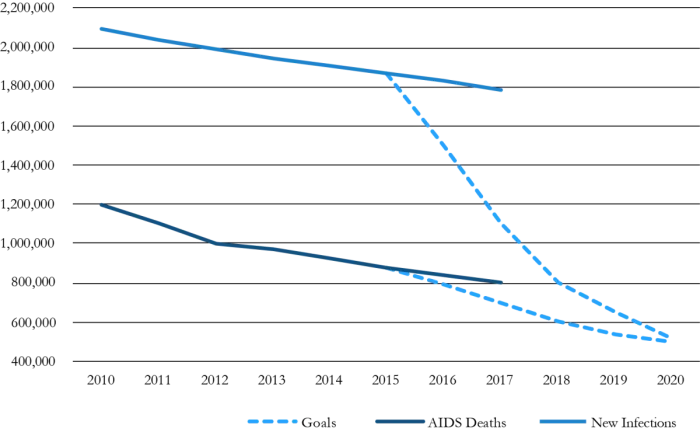
Yet progress is slipping as growing pandemics have been met with flat or reduced funding.22 HIV remains the leading global cause of death among people 15–49.14 Figure 2 shows trends are far off track from goals set at the UN General Assembly in 2016.23 Too many countries are experiencing rising infections (e.g., Brazil), AIDS deaths (e.g., Angola), or both (e.g., the Philippines). Malaria is on the rise globally and declines in TB have been far smaller than hoped.24 Drug-resistant TB and malaria are an international threat.25 Even as some countries approach malaria elimination, 20 of the highest-burden countries saw significant increases in cases.
U.S. foreign policy could contribute toward getting these efforts back on track— with financing and smart diplomacy. First, funding is key. Recent U.S. presidential budget proposals have sought cuts to the U.S. funding (figure 7). Growing pandemics require increased resources. Key innovations, from new TB treatments, to combination HIV prevention, to community case management for malaria could be scaled immediately, but lack resources. Second, increased multilateralism is needed. The UN, Global Fund, and other institutions provide necessary leverage for inter-governmental and civil society collaboration, making bilateral programs like PEPFAR far more effective, but need a greater share of U.S. political and financial support. Third, active U.S. diplomacy with other wealthy nations is needed since LMICs are increasing their investment but are met with donor reductions.26 Fourth, diplomatic policy engagement can support rights and evidence-based policies that make money effective. Criminalization of same-sex relationships, for example, is a major barrier to addressing HIV. The State Department has an office of “health diplomacy” that could be given an explicit mission to support law-reform and human rights efforts including effective strategic litigation.27
Keeping Tomorrow’s Outbreaks from Becoming Pandemics: Global Health Security
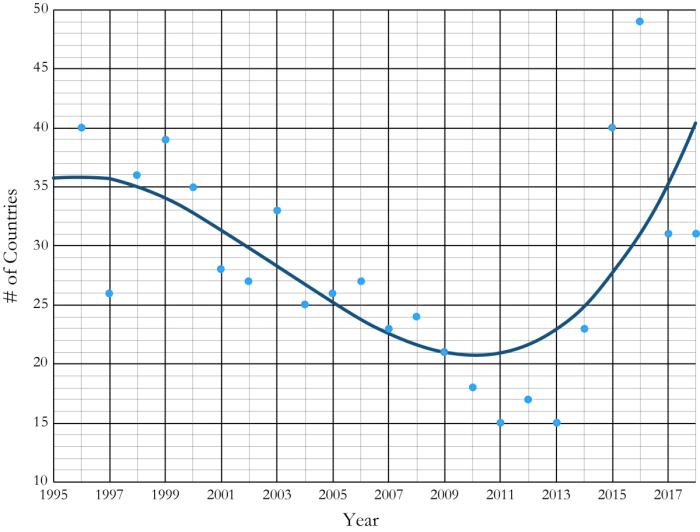
Since the West Africa Ebola epidemic, the WHO, the National Academy of Medicine and others have pointed to the major gaps in ensuring all countries can prevent, detect and respond to outbreaks.28 Today, a pathogen like influenza has the potential to travel around the world within hours and could kill tens of millions of people, disrupt economies, and destabilize national security.29 Modelers predict the emergence of an airborne virus of this sort sometime in the next 10 to 15 years.30 The number and diversity of disease outbreaks has increased significantly since 1980, even controlling for differences in reporting.31 Figure 3 shows an analysis of WHO reports on the number of countries experiencing outbreaks in a given year.32 Climate change, globalization, urbanization, migration, conflict, and antimicrobial resistance contribute to the intensification.
Strengthening U.S. capacity remains urgent.33 But a wider view based on justice and global interconnection suggests that protecting Americans from global hazards is best accomplished through partnerships to strengthen health systems. The Global Health Security Agenda (GHSA), launched in 2014 with strong U.S. support has focused on building core health-system capacities. It has grown to over 60 member countries and marshalled extensive resources, including U.S. investments in 17 target countries. The WHO’s Joint External Evaluation (JEE) has provided detailed evaluations of health security capacity in approximately 100 countries.
Progress, however, has been far too slow. Many countries still do not have sufficient capacity to prevent, detect, and respond to outbreaks, as demonstrated by JEE results.34 Future U.S. financing is uncertain even for the current 17 countries, while a significantly expanded set of countries needs support. The WHO’s Contingency Fund for Emergencies has consistently received far less than the $100 million requested, with nearly all of the funding in 2019 spent to fight Ebola.
U.S. policy on global pandemic preparedness could address several opportunities. First, programs like the Centers for Disease Control and Prevention’s Global Disease Detection program have proven highly effective in expanding lab, surveillance, and human resource capacity in LMICs, but are hampered by insufficient resources.35 Second, improving synergies across U.S.—supported programs could strengthen resilient systems if White House leadership prioritized cross-agency planning. There are promising examples. U.S. supported emergency operations for Ebola were recently expanded to prevent vertical transmission of HIV in Uganda, while health workers trained in Nigeria to fight HIV, TB, and polio were critical in responding to Ebola.36 Finally, with the need for U.S. support for global health emergencies growing, normalizing infrastructure and financing can help increase effectiveness of available response.
Preparing for and Preventing Climate-Sensitive Disease Outbreaks
Climate change is already causing illnesses and deaths, with risks projected to increase as climate change progresses.37 To avert increased health impacts, policies to curtail warming of the planet must be enacted. Meanwhile, preparing for and responding to rising risks of pandemic diseases are a critical component of effective climate policy.38 Poor and marginalized communities in LMICs will bear much of the burden.
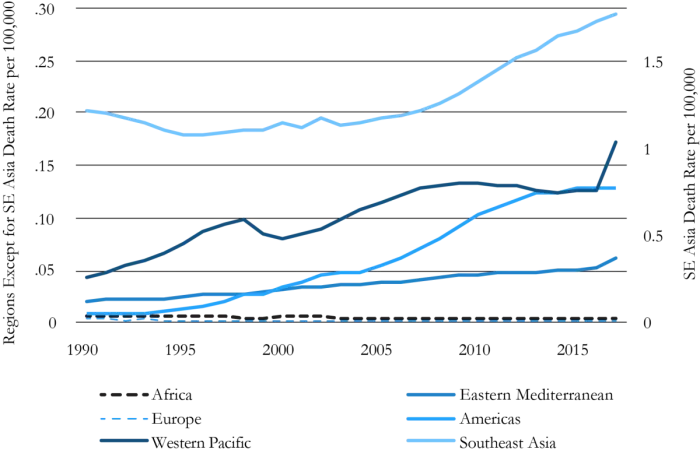
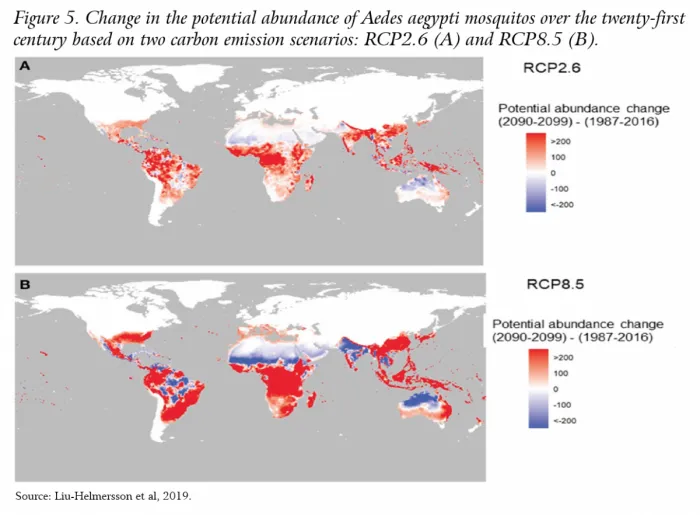
Weather and climate affect the geographic range, seasonality, and intensity of vector-borne diseases.39 Overall, the effect on infectious diseases can be hard to forecast and depends on the degree of warming and local ecology.40 Mosquito-borne diseases such as malaria, dengue, yellow fever, chikungunya, and Zika viruses are likely to reach larger populations, with greater effect at higher levels of warming and with significant regional variation.41 Death rates from dengue, one major mosquito-borne virus, have already increased significantly and climate trends are one factor.42 Figure 4 uses data from the Global Burden of Disease43 study to compile trends in death rates from dengue. The Lancet Countdown project linked this to expanded range and capacity for transmission of Aedes aegypti mosquitos, which have expanded by 3% since 1990 and are set to expand even further, according to modeling by Liu-Helmersson shown in figure 5.44 The public health emergency caused by the Zika pandemic of 2015–16 illustrates what happens as vector-borne diseases move into new regions with naïve populations.
Severe storms and flooding linked to climate change in areas with poor infrastructure are likely to drive water-borne diseases like cholera—as seen in Mozambique recently.45 By 2060, up to 400 million people could be affected by extreme flooding events, with associated risks of infectious diseases.46 Hundreds of millions may be vulnerable to displacement by the end of the century47—increasing the spread of infectious diseases if overcrowding and lack of safe water, food, and shelter are not addressed.48 Undernutrition has been identified as a major health impact of climate change, which increases risks from infectious disease.49 Marginalization based on gender, sexuality, and poverty will exacerbate these effects. Women’s and girls’ nutrition, for example, tends to suffer more during periods of scarcity, because they may be last in household food hierarchies.50
U.S. foreign policy could prioritize climate adaptation and mitigation efforts that address infectious disease in LMICs. First, making use of increasingly robust climate projections, global health aid could be partly targeted to regions expected to experience increases in range, seasonality, and/or intensity of disease because of climate change. Investments in early warning systems to predict outbreaks alongside multi-use laboratory capacity and human resources could create synergies across pandemic-related U.S. programs that support climate adaptation and mitigation. Second, U.S. foreign policy could support multilateral financing efforts for health sector adaptation including through the Green Climate Fund (for which U.S. funding was cut under the current administration). Just $9 million out of over $1.5 billion of climate funding from multilateral agencies recently went to health.51
Economic Impacts
A growing number of studies document the economic costs of infectious disease, with the largest cost coming from current pandemics. LMICs are home to over a third of global GDP and are a major U.S. trading partner, including the fastest growing economies.52 U.S. economic health is linked to this global growth.53
Economic effects of disease start at the individual level. Malaria cases in Nigeria, for example, reduce weekly earnings by 10–15%, while testing and treatment increase earnings and productivity.54 At the national level, the WHO Commission on Macroeconomics and Health and follow-up studies show that better health is linked to GDP growth.55
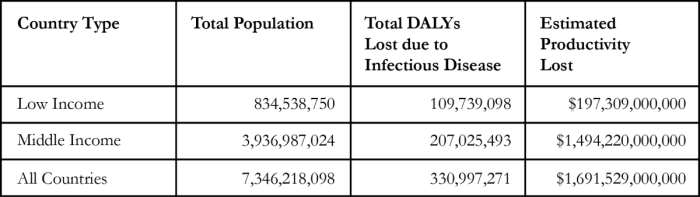
To estimate the productivity costs associated with morbidity and premature mortality due to infectious diseases in LMICs, we used an analytic framework used by the WHO.56 We determined the productivity losses for a given country by multiplying the estimated number of disability-adjusted life years (DALYs) lost due to infectious diseases by the monetary value of a full year of health without any illness. That monetary value was imputed using GDP per capita minus the total health expenditure per capita in the country. Data on health expenditures, DALYs, and GDP were obtained from publicly available databases.57
Overall, infectious diseases are responsible for over 300 million DALYs lost in LMICs, and we estimate that this costs $1.695 trillion in lost productivity (table 1). We find that the losses of 95.7% of Disability-Adjusted Life Years (DALYS) due to infectious diseases are in LMICs, even though these countries account for 65% of the world’s population. (See annex 1 for more details on methods and country-level estimates.)
New outbreaks are particularly harmful and act as shocks to the economies affected. The World Bank estimated that the Ebola pandemic in Sierra Leone, Liberia, and Guinea cost $2.2 billion in 2015 alone. The cost of future pandemics like novel influenza would be higher, and estimates range from $60 billion to $80 billion.58 Income represents only part of the loss from a pandemic; approaches that also value the lives lost find much larger impacts, at $500 billion, or 0.6% of global income per year.59
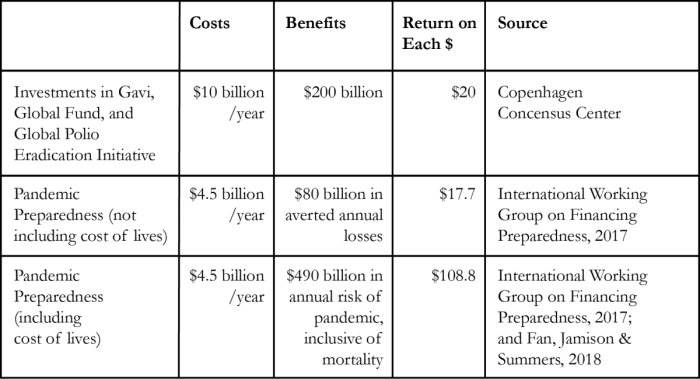
Meanwhile, strategic investments in a coordinated global-pandemics initiative would likely have a return ratio of between $17 and $20 on every $1 spent (table 2). The returns could be even higher, exceeding $100 per dollar, if the value of lives is included. Therefore, each $1 billion increase in investment could generate around $20 billion in returns to the global economy. This is highly consistent with a consensus that has emerged about the importance of investing in human capital.60 Increasing pandemic-related global health funding, then, represents a high-return opportunity that not only saves lives but also could bolster the global economy.
U.S. Financing to Fight Pandemics
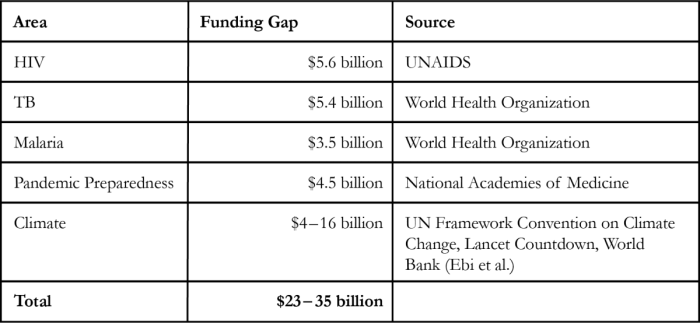
The global gap between available and needed funding for pandemic-related global health challenges in LMICs is approximately $23–35 billion annually. This includes $14.5 billion for AIDS, TB, and malaria,62 and $4.5 billion for pandemic preparedness.63 Between $4–15 billion is estimated to be needed annually for climate-related health adaptation, yet only about $0.04 billion in development funding is available.64
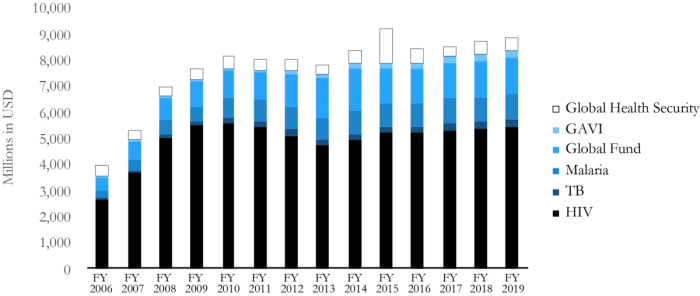
To understand the U.S. investment in pandemic-related global health, we analyzed funding from the U.S. government from 2006 through 2019—which spans the administrations of Presidents Bush, Obama, and Trump. Data were gathered from final, enacted appropriations bills.65 Included in this analysis were funding to USAID, the CDC, the Department of Defense, and the Department of State for HIV, TB, malaria, global health security, and global vaccine efforts through Gavi. We do not include, in this particular calculation, necessary investments in overall global health infrastructure, including to the National Institutes of Health and to child health, family planning funding, and other accounts. We also analyzed each presidential budget request from fiscal years 2010 to 2019 compared with the final enacted amounts.
$8.86 billion, or 0.19% of the U.S. federal budget, was appropriated in fiscal year 2019 for pandemic-related global health programs (figure 7). Little global health spending is used to address climate-sensitive disease, with no dedicated funding account (though needed programs could be funded through existing mechanisms).
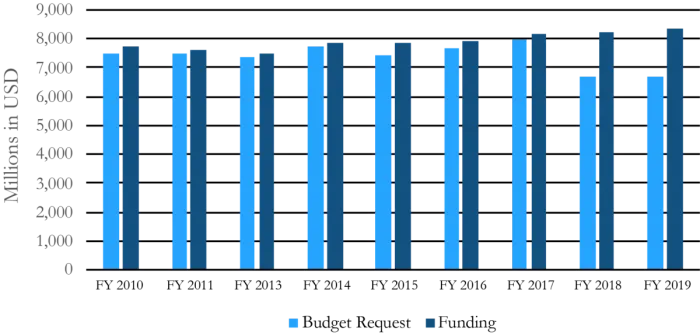
Figure 7 shows the substantial growth in funding during the Bush administration, with the launch of PEPFAR—illustrating the role of presidential leadership. In recent years, funding for these programs increased only incrementally. In the first years of the Trump administration, the president has requested significantly less than Congress has appropriated (Figure 8). This shows strong congressional support, but that only small increases have been politically feasible without White House leadership.
Structuring Expanded U.S. Government Effort
As described above, the U.S. has made significant global investments in funding and political effort in several of our key focus areas—from CDC programs on pandemic preparedness to PEPFAR and many other efforts. Multiple works and commissions have explored or are now exploring the current architecture and future directions.66 Here we focus on a narrower proposition: how might a sharpened, expanded U.S. foreign policy strategy on pandemics, with high–level political support, be shaped to realize the possibilities described above?
First, health aid is particularly effective when it focuses on clear targets, gaps in capacity that other actors cannot fill, and a clear mission. Presidential leadership has proven particularly important for programs like PEPFAR and PMI, particularly in setting clear targets and incentivizing cross-agency work. Such efforts result not just in lives saved but “soft power” diplomacy and improved opinion of the U.S.67 Therefore one key shift in foreign policy could be to set specific, linked goals for “pandemics” as a whole that allow research and interventions to cut across agencies and link diplomatic, programmatic, and aid activities together.
Second, there is a set of cross-cutting areas where the U.S. government is particularly well positioned to have impact. Health workforce is key, with a current shortage to reach international goals projected at 14 million workers by 2030.68 Programs like the CDC’s Field Epidemiology Training Program, which builds surveillance and response capacity in LMICs, could be expanded,69 alongside funding to recruit, train, and employ community health workers.70 Workers recruited to respond to HIV or TB, for example, can respond to new outbreaks.71 Investing in laboratories is another cross-cutting priority—building capacities from monitoring HIV, to identifying drug resistant TB, to diagnosing Ebola. Surveillance along with early warning and risk modeling systems could bring together “big data” on the environment, population, and disease to target resources and save lives, particularly as risks increase under climate change.72 Deploying new technologies quickly, affordably, and accessibly in LMICs could be a particular U.S. contribution to a global effort—from cutting–edge vaccines and medicines spurred by NIH funding to drone technology for transporting laboratory samples, which is already being tested in the deserts of Arizona.73
Third, a more multilateral approach has the potential to increase U.S. impact in ways, synergistic with bilateral efforts. The Global Fund is a good example where U.S. investment leverages leadership from governments and civil society in the Global North and South in ways that build democratic institutions, and civil society space.74 A new pandemics initiative could set a specific goal for increasing investment of dollars and collaboration in multilateral efforts through the U.N. and innovative financing institutions.
Finally, a specific set of shifts in U.S. foreign policy would be important. Engaging fully with U.N. activities and with global climate negotiations will be critical, as will shifting U.S. trade policy to support affordable medicines and supporting reform of the IMF and World Bank practices that undermine health systems. Eliminating policies that undercut the effectiveness of global health aid, like the ban on U.S. funding to groups that support abortion, is also key.75
Conclusion
Action on pandemics is urgent. Time is short to get the AIDS, TB, and malaria responses back on track, build capacity to keep the inevitable next outbreaks from becoming pandemics, and adapt to the rising threat of climate-linked diseases. U.S. action on global pandemics could help return some of the $1.7 trillion currently lost due to infectious disease in LMICs to the global economy. In a context of rising global inequality, halting pandemics also addresses shared global challenges. With pandemic-related global health programs making up just 0.19% of the U.S. budget, increased resources and policy shifts could make a significant impact. Doing so would also be a powerful signal that reducing risks to American wellbeing is best, and most justly, accomplished through global engagement and smart global health investments.
Matthew Kavanagh, PhD, is Director of the Global Health Politics & Policy Initiative at the Georgetown University O’Neill Institute for National and Global Health Law and a member of Georgetown’s Global Health and Law faculties.
Harsha Thirumurthy, PhD, is Associate Professor of Medical Ethics & Health Policy at the Perelman School of Medicine and Associate Director of the Center for Health Incentives and Behavioral Economics (CHIBE) at the University of Pennsylvania.
Rebecca Katz, PhD, MPH, Georgetown University is a Professor and Director of the Center for Global Health Science and Security. She was previously a consultant to the U.S. Department of State, working on issues related to the Biological Weapons Convention, pandemic influenza and disease surveillance.
Kristie L. Ebi, PhD, MPH, is a Professor in the Department of Global Health at the University of Washington. She has been conducting research and practice on the health risks of climate variability and change for nearly 25 years.
Chris Beyrer, MD, MPH, is the Desmond M. Tutu Professor of Public Health and Human Rights at the Johns Hopkins Bloomberg School of Public Health where he is Director of the Training Program in HIV Epidemiology & Prevention Science and Director of the Center for Public Health and Human Rights. He is the past president of the International AIDS Society.
Jamila Headley, MSc, PhD, is the Managing Director of the Health Global Access Project (Health GAP). She has a PhD in Public Health from Oxford University, where she studied as a Rhodes Scholar.
Charles B. Holmes, MD, MPH, is Faculty Co-Director of the Center for Global Health Practice and Impact and Visiting Associate Professor at Georgetown University and Associate Professor of Medicine at Johns Hopkins University. He was previously Chief Medical Officer for the U.S. President’s Emergency Plan for AIDS Relief in the U.S. Department of State.
Chris Collins, MPP, is President of Friends of the Global Fight Against AIDS, Tuberculosis and Malaria.
Lawrence O. Gostin, JD, is University Professor and Faculty Director at the Georgetown University O’Neill Institute for National and Global Health Law.
*Corresponding Author: Matthew M. Kavanagh, PhD, Georgetown University, O’Neill Institute for National & Global Health Law, 600 New Jersey Avenue NW, Washington DC 20001 USA ([email protected])
Acknowledgements: The authors wish to acknowledge Dr. Jennifer Kates and the Kaiser Family Foundation for contributing data on U.S. budgets and the research assistance of Matthew Boyce, Alexander Massaro, Nick Townsend, and Benny Chan.
NOTES
1 Richard Horton, “Offline: A President, Undone by Prejudice,” The Lancet 389, no. 10068 (2017): 489; Kristine M. Gebbie, “The President’s Commission on AIDS: What Did It Do?,” American Journal of Public Health 79, no. 7 (1989): 868–70; John W. Dietrich, “The Politics of PEPFAR: The President’s Emergency Plan for AIDS Relief,” Ethics & International Affairs 21, no. 3 (2007): 277–92.
2 Lawrence O. Gostin, Henry A. Waxman, and William Foege, “The President’s National Security Agenda: Curtailing Ebola, Safeguarding the Future,” JAMA 313, no. 1 (2015): 27–28.
3 Lawrence O. Gostin, Matthew M. Kavanagh, and Elizabeth Cameron, “Ebola and War in the Democratic Republic of Congo: Avoiding Failure and Thinking Ahead,” JAMA 321, no. 3 (2019): 243–44.
4 The definition of “pandemic” is widely debated. We use the term following David M. Morens, Gregory K. Folkers, and Anthony S. Fauci, “What Is a Pandemic?,” Journal of Infectious Diseases 200, no. 7 (2009): 1018–1021. Overall, this piece speaks to infectious diseases that are, by any measure, pandemics (e.g. HIV) as well as some that might be debated (e.g. TB in Southern Africa) as well as diseases that could become pandemic.
5 Christopher Dye, “After 2015: Infectious Diseases in a New Era of Health and Development,” Philosophical Transactions of the Royal Society B: Biological Sciences 369, no. 1645 (2014): 20130426; Dominique Tabutin et al., “Mortality Inequalities and Trends in Low-and Middle-Income Countries, 1990-2015,” Population 72, no. 2 (2017): 221–96; Thomas J. Bollyky et al., “Lower-Income Countries That Face the Most Rapid Shift in Noncommunicable Disease Burden Are Also the Least Prepared,” Health Affairs 36, no. 11 (2017): 1866–75.
6 Ben Oppenheim and Gavin Yamey, “Pandemics and the Poor,” Brookings Institution Future Development, June 19, 2017, https://www.brookings.edu/blog/future-development/2017/06/19/pandemics-and-the-poor/.
7 UNAIDS, “Global AIDS Update 2018: Miles To Go” (Geneva: UNAIDS, 2018).
8 Mosoka P. Fallah et al., “Quantifying Poverty as a Driver of Ebola Transmission,” PLoS Neglected Tropical Diseases 9, no. 12 (2015): e0004260.
9 Tedros Ghebreyesus, “Can We Create a Pandemic-Free World?” (February 12, 2018), http://www.who.int/dg/speeches/2018/pandemic-free-world/en/.
10 Peter Sands et al., “Outbreak Readiness and Business Impact: Protecting Lives and Livelihoods across the Global Economy” (Boston, MA: Harvard Global Health Institute & World Economic Forum, n.d.).
11 Sadie J. Ryan et al., “Global Expansion and Redistribution of Aedes-Borne Virus Transmission Risk with Climate Change,” PLoS Neglected Tropical Diseases 13, no. 3 (2019): e0007213.
12 M. J. Friedrich, “UN: All-out Effort Needed to Combat Antimicrobial Resistance,” JAMA 321, no. 23 (2019): 2273–2273.
13 Thomas Mann, A Question of Balance: The President, the Congress and Foreign Policy (Brookings Institution Press, 2010).
14 Joseph S. Nye Jr, “The Rise and Fall of American Hegemony from Wilson to Trump,” International Affairs 95, no. 1 (2019): 63–80.
15 International Monetary Fund, “World Economic Outlook Database” (Washington, DC: IMF, 2019), https://www.imf.org/external/pubs/ft/weo/2019/01/weodata/index.aspx; Gary Clyde Hufbauer and Zhiyao Lucy Lu, “The Payoff to America from Globalization: A Fresh Look with a Focus on Costs to Workers” (Washington, DC: Peterson Institute for International Economics, 2017), https://www.piie.com/publications/policy-briefs/payoff-america-globalization-fresh-look-focus-costs-workers.
16 Institute for Health Metrics and Evaluation, “Global Burden of Disease,” 2019, https://vizhub.healthdata.org/gbd-compare/.
17 UNAIDS, “The GAP Report” (UNAIDS, 2014), https://www.unaids.org/en/resources/campaigns/2014/2014gapreport/gapreport.
18 UNAIDS, “2019 Global AIDS Update: Communities at the Centre” (Geneva: UNAIDS, 2019).
19 World Health Organization (WHO), “Global Tuberculosis Report 2018” (Geneva: WHO, 2018); World Health Organization, “World Malaria Report 2018” (Geneva: WHO, 2018).
20 N. Hamunime et al., “Progress toward HIV Epidemic Control: Results from the Namibia Population-Based HIV Impact Assessment (PHIA),” in Journal of the International AIDS Society, vol. 21, 2018, 167–167.
21 United Nations, “Political Declaration on HIV and AIDS: On the Fast-Track to Accelerate the Fight against HIV and to End the AIDS Epidemic by 2030.,” A/70/L.52 § (2016); Office of the UN Secretary-General’s Special Envoy for Financing the Health Millennium Development Goals for Malaria, “From Aspiration to Action: What Will It Take to End Malaria?,” 2015; World Health Organization, “The End TB Strategy” (Geneva: WHO, 2014).
22 Jennifer Kates, Adam Wexler, and Eric Lief, “Donor Government Funding for HIV in Low- and Middle-Income Countries in 2018” (Washington, DC: Kaiser Family Foundation & UNAIDS, 2019).
23 UNAIDS, “AIDSinfo,” n.d., http://aidsinfo.unaids.org/; UNAIDS, “Fast-Track - Ending the AIDS Epidemic by 2030” (Geneva: UNAIDS, December 1, 2014).
24 World Health Organization, “World Malaria Report 2018”; World Health Organization (WHO), “Global Tuberculosis Report 2018.”
25 World Health Organization (WHO), “Global Tuberculosis Report 2018”; World Health Organization, “World Malaria Report 2018”; F. Castelli and G. Sulis, “Migration and Infectious Diseases,” Clinical Microbiology and Infection 23, no. 5 (2017): 283–89; Robinson Jaramillo-Ochoa et al., “Effects of Political Instability in Venezuela on Malaria Resurgence at Ecuador–Peru Border, 2018,” Emerging Infectious Diseases 25, no. 4 (2019): 834; Asad Mustafa Karim et al., “Epidemiology and Clinical Burden of Malaria in the War-Torn Area, Orakzai Agency in Pakistan,” PLoS Neglected Tropical Diseases 10, no. 1 (2016): e0004399; P. Dhavan et al., “An Overview of Tuberculosis and Migration,” The International Journal of Tuberculosis and Lung Disease 21, no. 6 (2017): 610–23.
26 UNAIDS, “2019 Global AIDS Update: Communities at the Centre.”
27 Allan Yuhas, “A Win for Gay Rights in Botswana Is a ‘Step Against the Current’ in Africa - The New York Times,” New York Times, June 11, 2019, https://www.nytimes.com/2019/06/11/world/africa/ botswana-gay-homosexuality.html; Ryan Thoreson, “Lesbian, Gay, Bisexual, Transgender, Queer, and Intersex (LGBTQI) Rights and Sub-Saharan Africa,” in Oxford Research Encyclopedia of Politics, 2018.
28 Lawrence O. Gostin et al., “Toward a Common Secure Future: Four Global Commissions in the Wake of Ebola,” PLoS Medicine 13, no. 5 (2016): e1002042; International Working Group on Financing Preparedness, “From Panic and Neglect to Investing in Health Security: Financing Pandemic Preparedness at a National Level.” (Washington, DC: World Bank, 2017); Steven J. Hoffman and Sarah L. Silverberg, “Delays in Global Disease Outbreak Responses: Lessons from H1N1, Ebola, and Zika,” American Journal of Public Health 108, no. 3 (2018): 329–33.
29 Global Preparedness Monitoring Board, “World At Risk: Annual Report on Global Preparedness for Health Emergencies” (Geneva, 2019), https://apps.who.int/gpmb/annual_report.html; Lisa Monaco and Vin Gupta, “The Next Pandemic Will Be Arriving Shortly,” Foreign Policy, September 28, 2018, https://foreignpolicy.com/2018/09/28/the-next-pandemic-will-be-arriving-shortly-global-health-infectious-avian-flu-ebola-zoonotic-diseases-trump/.
30 Bill Gates, “Innovation for Pandemics,” New England Journal of Medicine 378, no. 22 (2018): 2057–60.
31 Katherine F. Smith et al., “Global Rise in Human Infectious Disease Outbreaks,” Journal of The Royal Society Interface 11, no. 101 (2014): 20140950.
32 World Health Organization, “Disease Outbreak News (DONs)” (Geneva: WHO, 2019), https:// www.who.int/csr/don/archive/year/en/.
33 Barbara J. Jester et al., “100 Years of Medical Countermeasures and Pandemic Influenza Preparedness,” American Journal of Public Health 108, no. 11 (2018): 1469–72.
34 Vin Gupta et al., “Analysis of Results from the Joint External Evaluation: Examining Its Strength and Assessing for Trends among Participating Countries,” Journal of Global Health 8, no. 2 (2018).
35 Joel M. Montgomery et al., Ten Years of Global Disease Detection and Counting: Program Accomplishments and Lessons Learned in Building Global Health Security (BioMed Central, 2019).
36 Tom Daschle and Bill Frist, “The Case for Strategic Health Diplomacy: A Study of PEPFAR” (Washington, DC: Bipartisan Policy Center, 2015).
37 Kristie L. Ebi et al., “Detecting and Attributing Health Burdens to Climate Change,” Environmental Health Perspectives 125, no. 8 (2017): 085004; U.S. Global Change Research Program, “Fourth National Climate Assessment Volume II: Impacts, Risks, And Adaptation” (Washington, DC, 2018), https://nca2018.globalchange.gov/.
38 Nick Watts et al., “Health and Climate Change: Policy Responses to Protect Public Health,” The Lancet 386, no. 10006 (2015): 1861–1914.
39 Cory W. Morin, Andrew C. Comrie, and Kacey Ernst, “Climate and Dengue Transmission: Evidence and Implications,” Environmental Health Perspectives 121, no. 11–12 (2013): 1264–72.
40 Zhoupeng Ren et al., “Predicting Malaria Vector Distribution under Climate Change Scenarios in China: Challenges for Malaria Elimination,” Scientific Reports 6 (2016): 20604.
41 Andy Haines and Kristie Ebi, “The Imperative for Climate Action to Protect Health,” New England Journal of Medicine 380, no. 3 (2019): 263–73; Nick Watts et al., “The 2018 Report of the Lancet Countdown on Health and Climate Change: Shaping the Health of Nations for Centuries to Come,” The Lancet 392, no. 10163 (2018): 2479–2514.
42 Kristie L. Ebi and Joshua Nealon, “Dengue in a Changing Climate,” Environmental Research 151 (2016): 115–23.
43 Institute for Health Metrics and Evaluation, “Global Burden of Disease.”
44 Watts et al., “The 2018 Report of the Lancet Countdown on Health and Climate Change: Shaping the Health of Nations for Centuries to Come”; Jing Liu-Helmersson et al., “Estimating Past, Present, and Future Trends in the Global Distribution and Abundance of the Arbovirus Vector Aedes Aegypti Under Climate Change Scenarios,” Frontiers in Public Health 7 (2019).
45 Alistair J. Woodward and Jonathan M. Samet, Climate Change, Hurricanes, and Health (American Public Health Association, 2018); Melanie Boeckmann et al., “Climate Change and Control of Diarrhoeal Diseases in South Africa: Priorities for Action,” South African Medical Journal 109, no. 6 (2019): 359–61.
46 Barbara Neumann et al., “Future Coastal Population Growth and Exposure to Sea-Level Rise and Coastal Flooding-a Global Assessment,” PloS One 10, no. 3 (2015): e0118571.
47 Oli Brown, Migration and Climate Change (International Organization for Migration, 2008).
48 The Intergovernmental Panel on Climate Change, “Climate Change and Land: An IPCC Special Report on Climate Change, Desertification, Land Degradation, Sustainable Land Management, Food Security, and Greenhouse Gas Fluxes in Terrestrial Ecosystems” (United Nations, 2019).
49 Maryia Bakhtsiyarava, Kathryn Grace, and Raphael J. Nawrotzki, “Climate, Birth Weight, and Agricultural Livelihoods in Kenya and Mali,” American Journal of Public Health 108, no. S2 (2018): S144–50.
50 World Health Organization, Gender, Climate Change and Health (World Health Organization, 2014).
51 World Health Organization, “COP24 Special Report: Health & Climate Change” (Geneva: WHO, 2018).
52 United Nations, World Economic Situation and Prospects (New York: United Nations Publications, 2019), https://www.un.org/development/desa/dpad/publication/world-economic-situation-and-prospects-as-of-mid2019/; World Bank, “The World Bank In Middle Income Countries,” accessed July 18, 2019, https://www.worldbank.org/en/country/mic/overview.
53 Ayhan Kose et al., The Global Role of the US Economy: Linkages, Policies and Spillovers (The World Bank, 2017); Hufbauer and Lu, “The Payoff to America from Globalization: A Fresh Look with a Focus on Costs to Workers.”
54 Andrew Dillon, Jed Friedman, and Pieter Serneels, Health Information, Treatment, and Worker Productivity: Experimental Evidence from Malaria Testing and Treatment among Nigerian Sugarcane Cutters (The World Bank, 2014).
55 Jeffrey D. Sachs, Macroeconomics and Health: Investing in Health for Human Development (Geneva: World Health Organization, 2001); Alok Bhargava et al., “Modeling the Effects of Health on Economic Growth,” Journal of Health Economics 20, no. 3 (2001): 423–40; David E. Bloom, David Canning, and Dean T. Jamison, “Health, Wealth, and Welfare,” Finance and Development 41 (2004): 10–15; Hoyt Bleakley, “Health, Human Capital, and Development,” Annu. Rev. Econ. 2, no. 1 (2010): 283–310.
56 World Health Organization, “A Heavy Burden: The Productivity Cost of Illness in Africa,” 2019; Juliet Nabyonga Orem et al., “Impact of Malaria Morbidity on Gross Domestic Product in Uganda,” International Archives of Medicine 5, no. 1 (2012): 12; Joses M. Kirigia et al., “Indirect Cost of Maternal Mortality in the WHO African Region, 2013,” International Journal of Social Economics 43, no. 5 (2016): 532–48.
57 World Health Organization, “Global Health Observatory,” 2019, http://www.who.int/gho/database/ en/; International Monetary Fund, “World Economic Outlook Database.”
58 Warwick J. McKibbin and Alexandra Sidorenko, Global Macroeconomic Consequences of Pandemic Influenza (Lowy Institute for International Policy Sydney, Australia, 2006).
59 Victoria Y. Fan, Dean T. Jamison, and Lawrence H. Summers, “Pandemic Risk: How Large Are the Expected Losses?,” Bulletin of the World Health Organization 96, no. 2 (2018): 129.
60 Jim Yong Kim, “Eliminating Poverty in the 21st Century: The Role of Health and Human Capital,” JAMA 320, no. 14 (2018): 1427–28; World Bank, “The Human Capital Project” (Washington, DC: World Bank, 2018).
61 Copenhagen Consensus Center, “Health: Infectious Diseases Benefits and Costs for the Post-2015 Development Agenda” (Copenhagen, n.d.), https://www.copenhagenconsensus.com/post- 2015-consensus/health-infectious-diseases; Bill Gates, “The Best Investment I’ve Ever Made,” Wall Street Journal, January 19, 2019, https://www.wsj.com/articles/bill-gates-the-best-investment-ive-ever-made-11547683309; International Working Group on Financing Preparedness, “From Panic and Neglect to Investing in Health Security”; Victoria Y. Fan, Dean T. Jamison, and Lawrence H. Summers, “Pandemic Risk: How Large Are the Expected Losses?”
62 World Health Organization (WHO), “Global Tuberculosis Report 2018”; World Health Organization, “World Malaria Report 2018”; UNAIDS, “2019 Global AIDS Update: Communities at the Centre.”
63 International Working Group on Financing Preparedness, “From Panic and Neglect to Investing in Health Security: Financing Pandemic Preparedness at a National Level.”
64 Watts et al., “The 2018 Report of the Lancet Countdown on Health and Climate Change: Shaping the Health of Nations for Centuries to Come”; UNFCC, “United Nations Framework Convention on Climate Change” (U.N. Doc. A/AC.237/18 (Part II)/Add.1; 31 ILM 849, 1992); Kristie L. Ebi, Jeremy J. Hess, and Paul Watkiss, “Health Risks and Costs of Climate Variability and Change,” in Disease Control Priorities, Third Edition (Volume 7) (Washington, DC: World Bank, 2017).
65 We recognize assistance from Jennifer Kates and the staff at Kaiser Family Foundation for helping gather and this data. Analysis presented below is original to this paper. See Kaiser Family Foundation Global Health Tracker for more information on US appropriations bills. https://www.kff. org/interactive/budget-tracker/
66 Kaiser Family Foundation, “The U.S. Government and Global Health” (Washington, DC: KFF, July 30, 2019), https://www.kff.org/global-health-policy/fact-sheet/the-u-s-government-and-global-health/; National Academy of Medicine, Global Health and the Future Role of the United States (Washington, DC: National Academies Press, 2017); Center for Strategic and International Studies, “Commission on Strengthening America’s Health Security,” CSIS, accessed September 25, 2019, https://healthsecurity.csis.org/.
67 Tom Dashle et al., “Building Prosperity, Stability, and Security Through Strategic Health Diplomacy: A Study of 15 Years of PEPFAR” (Washington DC: Bipartisan Policy Center, 2018); Aleksandra Jakubowski et al., “Impact of Health Aid Investments on Public Opinion of the United States: Analysis of Global Attitude Surveys From 45 Countries, 2002–2016,” American Journal of Public Health 109, no. 7 (2019): 1034–41.
68 World Health Organization, “Global Strategy on Human Resources for Health: Workforce 2030.” (Geneva: WHO, 2016); Michel Sidibé and James Campbell, Reversing a Global Health Workforce Crisis (SciELO Public Health, 2015); Wim Van Damme et al., Is the World Ready for the next Pandemic Threat? (British Medical Journal Publishing Group, 2018).
69 Donna S. Jones et al., “Building Global Epidemiology and Response Capacity with Field Epidemiology Training Programs,” Emerging Infectious Diseases 23, no. Suppl 1 (2017): S158.
70 Matthew R. Boyce and Rebecca Katz, “Community Health Workers and Pandemic Preparedness: Current and Prospective Roles,” Frontiers in Public Health 7 (2019): 62.
71 Tom Dashle et al., “Building Prosperity, Stability, and Security Through Strategic Health Diplomacy: A Study of 15 Years of PEPFAR.”
72 Watts et al., “The 2018 Report of the Lancet Countdown on Health and Climate Change: Shaping the Health of Nations for Centuries to Come.”
73 Timothy K. Amukele et al., “Drone Transport of Chemistry and Hematology Samples over Long Distances,” American Journal of Clinical Pathology 148, no. 5 (2017): 427–35.
74 Matthew M. Kavanagh and Lixue Chen, “Governance and Health Aid from the Global Fund: Effects Beyond Fighting Disease,” Annals of Global Health 85, no. 1 (2019).
75 Jerome A. Singh and Salim S. Abdool Karim, “Trump’s ‘Global Gag Rule’: Implications for Human Rights and Global Health,” The Lancet Global Health 5, no. 4 (2017): e387–89; David Stuckler et al., “An Evaluation of the International Monetary Fund’s Claims about Public Health,” International Journal of Health Services 40, no. 2 (2010): 327–32; Ellen ’t Hoen, Private Patents and Public Health: Changing Intellectual Property Rules for Access to Medicines (Health Action International, 2016).