The Strength of Weak Cities? Deconstructing COVID-19 in Urban Africa
Africa was once expected to be the heartland of COVID-19 cases and deaths—a monumental disaster waiting to happen. Yet, while Africa accounts for 17.2 percent of the world population, it thus far accounts for only 4 percent of COVID-19 deaths and 2.7 percent of cases globally. What does this appreciable disparity reveal or occlude about the management of public health emergencies in African cities? This essay explores lessons learned from addressing the COVID-19 pandemic in urban Africa, ranging from early and aggressive responses to community-led initiatives and sound public health policies derived from longstanding experience with infectious disease such as the Ebola epidemic. COVID-19, I argue, opens a critical space for defamiliarizing commonsense representations of African cities. We must move beyond the default assumption that “cities in Africa just don’t work” and instead pay critical attention to hybrid and adaptive governance systems emerging across urban Africa.
This essay appears in Vol. 74, No. 1, "Global Urbanization: Nations, Cities, and Communities in Transformation" (Fall/Winter 2021).
Africa is home to the most rapid urban growth in the world: the continent’s urban population increased tenfold between 1960 and 2020, from 53 million to 588 million.[1] Given that about 95 percent of COVID-19 cases occur in cities, and given the sobering realities that accompany Africa’s rapid urban growth, including subpar health care systems, expanding slums, and an intensifying informal economy, cases and deaths on the continent were once expected to surge and provoke a monumental disaster.[2] African cities were warned in the spring of 2020 to “prepare for the worst”[3] as they “stand [no] chance in the fight against COVID-19.”[4] One BBC News article ran the headline “Coronavirus: Africa could be the next epicenter.”[5] A France 24 headline read: “Vulnerable Continent: Africa and the Coronavirus.”[6] Presented as a fait accompli, these apocalyptic predictions reinforced tropes of endemic crisis and passivity that have cast a long shadow over how we think, write, and teach about urban Africa. The common denominator for these fixed and linear framings is the failure to parse the African city as a primary site of agency, collective organizing, resourcefulness, and possibility.
Yet, while Africa accounts for 17.2 percent of the world population, it accounted for only 2.7 percent of all COVID-19 cases globally as of March 2022. By comparison, North America accounted for 22 percent cases and Europe more than a third. Between then and February 14, 2020, when the first case on the continent was detected in Egypt, Africa recorded 251,754 deaths, about 42 percent of them in South Africa. Compare this to 1,017,010 deaths in Asia, 1,000,428 in North America, and 1,868,883 in Europe. Africa as a whole has experienced fewer COVID-19 deaths than France; even then, just five countries—South Africa, Tunisia, Egypt, Morocco, and Algeria—account for 60.6 percent of the continent’s reported cases and 71.2 percent of deaths.[7] What does this appreciable disparity reveal or occlude about the management of public health emergencies in African cities?
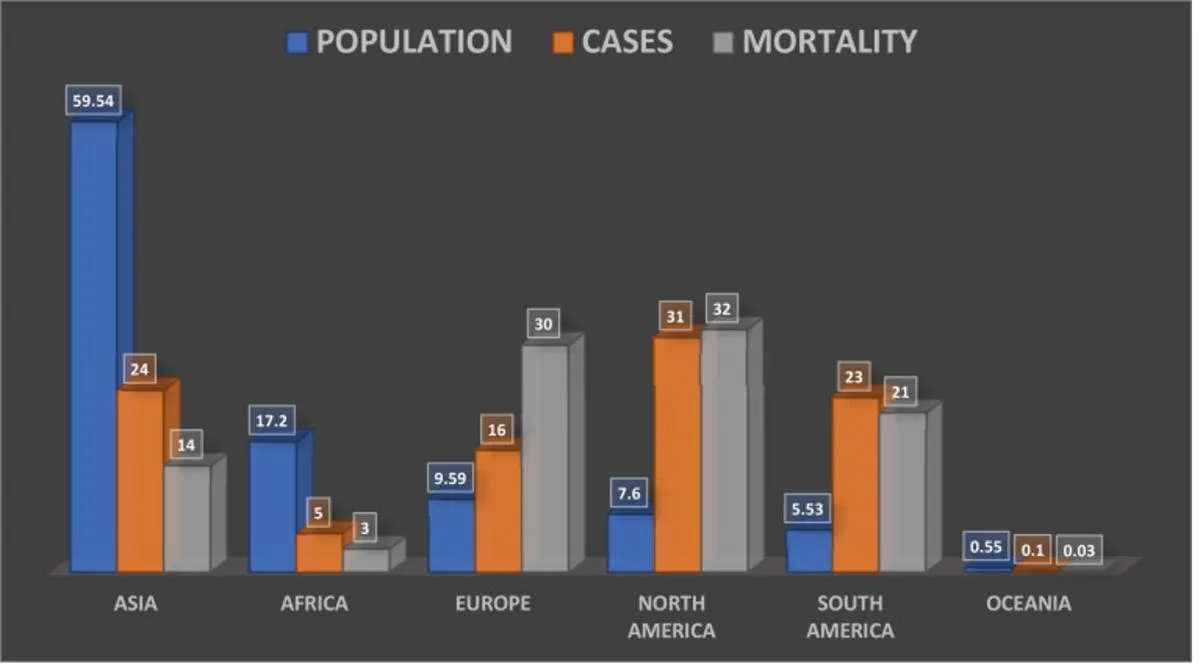
Figure 1: COVID-19 Cases and Mortality in Percentages in June 2021[8]
This essay explores lessons learned from addressing the pandemic in urban Africa, including early and aggressive responses, community-led initiatives, and sound public health policies derived from longstanding experience with infectious disease like the Ebola epidemic from 2013 to 2016. It argues that COVID-19 creates a critical space for a reality check, that is, for defamiliarizing commonsense representations of African cities. In doing so, the essay invites us to see familiar things in unfamiliar ways and in unlikely places. It begins by deconstructing ways of viewing African cities in the extant literature. It then offers a critique of journalistic coverage of the COVID-19 pandemic in Africa, taking examples from major global media outlets. Finally, it assesses timely and decisive steps taken by governments and local communities in Africa to contain the virus.
Deconstructing the African City
African cities typically emerge in the extant literature as extreme or exceptional; hopeless or hopeful. On the one hand, they are represented as bastions of expanding slums (where around 60 percent of the continent’s urban dwellers live), biting poverty, rising unemployment, and surplus humanity; in short, as places that fall short of the expectations of modernity, which is said to have its fons et origo in the West.[9] This dystopian reading reinforces colonial images of Africa as a wasteland dotted with crime, disease, and “dirty natives.”[10] Far from being passé, this tendency towards homogeneous and binarized representations of African cities is alive and well in today’s dominant analytical frameworks, which closely align Western cities with modernity and non-Western cities with developmentalism. African cities thus enter urban studies as not-quite-cities—as problems to be solved—and as cities struggling to acquire “world class” status. Lagos, for instance, brands itself as “Africa’s Big Apple,”[11] while Johannesburg promotes itself as a “world class African city.”[12] As anthropologists Jean Comaroff and John Comaroff argue, “To the degree that, from a Western perspective, the Global South is embraced by modernity at all, then, it is an outside that requires translation, conversation, catch-up.”[13] Relaxing this parochial practice of gazing at non-Western cities through Western lenses would require seeing Africa as people[14] and “people as infrastructure,”[15] which is to say, as products of social networks and inventive responses that animate the city.
Growing calls to move beyond Afropessimist discourses that view the African city as a basket case of multiple pathologies, what geologist Matthew Gandy calls the “aesthetic of chaos,” have opened a hopeful door for exceptional readings of the African city.[16] Such readings underscore the coping mechanisms, improvisations, and inventiveness of city dwellers in Africa, whose daily and defiant struggle for survival and recognition is interpreted as defying commonsense logic and Western notions of order. This viewpoint is exemplified by Rem Koolhaas, who sees the congestion and chaos of Lagos, Nigeria’s commercial capital and sub-Saharan Africa’s largest city, as revealing a hidden order. Far from being backward, says Koolhaas, Lagos is at the “forefront of a globalizing modernity.”[17] While this aesthetic framing usefully underscores the rise of new forms of urbanism in Africa, it overlooks dire realities facing the informal workforce that constitutes about 87 percent of employment in Africa, especially extortion, dispossession, and displacement.
Going beyond essentialist narratives that describe African cities as extreme or exceptional, this essay takes up the challenge posed by critical urbanists to defamiliarize ways of conceptualizing urban Africa that have ensured that the non-Western city is so fully eclipsed by an omnipotent Western city as to be rendered “inaudible, unspeaking, and unspeakable.”[18] Through a concretization of how governments and local communities in urban Africa have responded to the COVID-19 pandemic, it aims to do more than merely call for a “postcolonization” and “de-Westernization” of urban studies, but instead to reconstruct urban theory from a primarily non-Western perspective. In so doing, it shows why contemporary urban scholarship and policymaking should reconfigure African cities as complex, innovative, and adaptive human ecosystems. This entails engaging with African cities from a dynamic rather than static position, as well as seeing crisis in urban Africa as a terrain of action and meaning rather than simply as context.
Beyond the Headlines
News coverage of the COVID-19 pandemic in Africa has recycled colonial representations of the continent as both an imminent and an immanent threat, and city dwellers as both a risk and at risk. At the onset of the pandemic, the United Nations estimated that without government intervention, 1.2 billion Africans would be infected with the virus and 3.3 million would die. Even in the best-case scenario, where African governments strictly enforced lockdown and social distancing measures, the UN maintained that once a threshold of 0.2 deaths per 100,000 people per week was reached, the continent would experience 122.8 million infections, 2.3 million cases of hospitalizations, and 300,000 deaths.[19]Consequently, the UN called for a $100 billion safety net to mitigate the imminent doom about to strike Africa.
Patently, catastrophic predictions about the pandemic in Africa have not come to pass; at least, not yet. Puzzled by this, many analysts have floated conspiracy theories that cast the continent as a suspect community with a hidden smoking gun.[20] Meanwhile, the elephant in the room is largely ignored: What if some African cities, governments, and public health strategies have been more effective at addressing COVID-19 than those of the West? Put differently by the Comaroffs: “What if we posit that, in the present moment, it is the so-called ‘Global South’ that affords privileged insight into the workings of the world at large?”[21]
The coverage of infectious viral diseases in Africa—from HIV/AIDS to SARS and Ebola—is at its core apocalyptic and myopic, denying an entire continent of 54 countries any agency or capacity for action.[22] The narrative around COVID-19 follows a similar pattern. Take two characteristic stories of the BBC and New York Times, major media outlets in the United Kingdom and the United States, countries that paradoxically have had two of the highest COVID-19 infection and death rates in the world. On September 3, 2020, an article by BBC journalist and author Andrew Harding entitled “Coronavirus in Africa: Could poverty explain mystery of low death rate?” cited epidemiologists who suspected that Africa’s low death rates were due to its impoverished, crowded, and unhygienic neighborhoods, which were said to afford some level of pre-existing, cross-protective immunity against COVID-19. They theorized that other human coronaviruses, such as those that cause the common cold, might also elicit an immune response against COVID-19.[23] Were this supposition true, it would prompt the question: Why did we see exponential surges of COVID-19 in other densely populated nations with a similar combination of slums, such as Brazil and India?[24]
Harding’s piece both reproduces and upends the “outbreak narrative” that blames a pandemic’s spread on primitive ways of life and primordial spaces, resulting in the stigmatization of entire groups and places.[25] During the 2014 Ebola epidemic in Sierra Leone, some Western experts interpreted the lack of basic social amenities, overcrowded living and working conditions, and cultural practices like bushmeat consumption and burial practices as primary drivers of the spread of the infectious disease. By contrast, in South Africa, poor infrastructure and dense living conditions are repackaged as causal explanations for the low spread of COVID-19. The accumulation of these contradictory interpretations serves to reinforce the framing of African cities as emblems of the pathological and turns a blind eye to how the precarious existence of the African subaltern is closely entwined with Western colonialism, neoliberal capitalism, and global inequalities.
Harding’s piece sparked a public outcry on social media as Africans criticized its offensive and totalizing headline. One Twitter user noted, “Is this for real? It seems they always find a way to cover African news in a negative light. Even if it’s good news!”[26] Another user denounced the sweeping generalization of the headline: “Surely getting in voices from other parts of the continent, if you must generalize, would have been better… Otherwise change your headlines to the true focus: South Africa.”[27] In light of this criticism, the BBC retracted the headline, confirming in a tweet, “The headline and article have been updated to better reflect what the scientist said. It was not our intention to cause offence.”[28] The headline has been revised to “Coronavirus in South Africa: Scientists explore surprise theory for low death rate.”
Western media outlets sometimes attribute Africa’s lower-than-expected COVID-19 mortality rates to humid climatic conditions, as if humidity were homogeneous across the continent. If warm weather were an impediment to the spread of the virus, why has Brazil recorded more than 29 million COVID-19 cases and 655,000 deaths?[29] In the United States, a popular expectation held that the summer of 2020 would usher in some much-needed relief to spiraling infection and death rates. Yet the summer came and went without a substantial reduction in transmission rates. As the medical anthropologist Adia Benton pointedly notes: “Pseudo-explanations for a relatively low pandemic toll in Africa flow from the morbid expectation that any divergence or deviance from the norm—African sickness and death—is about what Africans are rather than what they did (or failed to do).”[30]
The above examples are not the exception, but the rule for how the hitherto low impact of COVID-19 in African cities has been interpreted. The organizing logic is simple and all too familiar: If Europe and North America have been hit hard by COVID-19 cases and deaths, then Africa stands no chance. In September 2020, the New York Post published an article with the headline, “Scientists can’t explain puzzling lack of coronavirus outbreaks in Africa.”[31] A New York Timespiece published on January 4, 2021 and headlined “A continent where the dead are not counted” soon took up the puzzle. Author Ruth Maclean claimed that death rates were low because of a lack of official registrations, citing UN data indicating that 90 percent of deaths are registered in Western countries and implying dramatically lower numbers in Africa without hard data.[32] The headline was not only misleading, but methodologically flawed. Selecting a couple of vague examples from Sudan and Nigeria out of a vast continent, the piece made a sweeping claim that the dead are not counted in Africa, reproducing the stereotype of Africa as a place of unprocessed data—as geographer Carolyn Gallaher writes, as an informational black hole that is “strangely devoid of agency and the possibility for enunciation, creative potential and communal action.”[33]
More nuanced reporting would have shown that while African countries—with the exception of Egypt, South Africa, Tunisia, Algeria, Cape Verde, Sao Tome and Principe, Seychelles, and Mauritius—lack a well-functioning civil registration and vital statistics system, which complicates the calculation of deaths, virtually all African countries have some sort of death registration system, such as verbal autopsies, whereby people close to the deceased help identify the cause of death.[34] The problem with the registration of deaths in many African cities is that they are paper-based and sometimes misplaced or lost.[35] It is true that COVID-19 testing rates are generally low in Africa. For instance, when Nigeria reported its first case on February 27, 2020, it had only five operational testing laboratories in four states. Irregular levels of testing can, over time, mask the actual spread of COVID-19. In fact, according to a former Red Cross official to whom I spoke in the city of Kano:
Nigeria’s health care system is nothing to write home about. A state governor was asked about his level of preparedness at the beginning of the pandemic and claimed he was fully prepared, like other states, and he has three intensive care unit beds in a state of over 3 million people… The number of people who tested positive in Nigeria are a mere fraction of the people with this virus, as there are questions regarding the capability of the government to effectively and efficiently test the population at risk.[36]
However, it remains a quantum leap to infer that the low death rate per capita in Africa is due to poor testing or to underreported deaths. How can it be that in a megacity such as Lagos—with a population almost three times greater than London’s, where residents live in crowded housing nicknamed “face-me-I-face-you,” and where the well of rumors never runs dry—tens of thousands of sudden, mysterious deaths could go unnoticed?[i] Growing up in Alimosho, the largest local government area in Lagos, I lived in a bungalow adjoining a face-me-I-face-you building. Hardly a death was missed, since people generally knew, and knew about, each other. If we are neither hearing residents of crowded urban housing talking about sudden, mysterious deaths nor seeing increased scenes of overwhelmed hospitals and unusual rises in funeral ceremonies across African cities,[ii] then claims of a “huge, hidden outbreak” on the continent should be tempered.[37] As the director for the Africa Centres for Disease Control (Africa CDC), John Nkengasong, points out: “We may not have been picking up all the [COVID-19] cases, just like in other parts of the world… but we are not seeing people around the continent falling dead on the streets or mass burials going on.”[38]
Such coverage of COVID-19 exemplifies what the writer Chimamanda Adichie calls “the danger of a single story,” which has long marked African cities as the perpetual exception to the rule of modernity.[39] The real newsworthy discussion is what lessons can be learned from the management of COVID-19 in African cities, not why so many deaths go under-recorded. Centering such one-sided questions on a continent bubbling with diversity reveals a perfunctory assumption, too often headlined by Western media outlets, that when the world has it bad, Africa must have it worse. Ignoring Africa’s agency and seeing it only in these apocalyptic terms reveals a clear failure to speak of non-Western cities in ways that warrant comparison with Western cities.[40] This habit reproduces entrenched imaginaries of African cities as residual entities that offer nothing of value to the study of world historical events or of the human condition writ large.[41] The most important question of the COVID-19 pandemic in Africa is not so much about the pedagogies of absence as of presence: What can Africa’s ability to swiftly adapt in the face of a deadly global pandemic teach us about the strength of so-called “weak” or “fragile” cities?
Learning from Africa
When my family wanted to travel from Nairobi to Tanzania [this winter], we required negative COVID-19 test results to be allowed entry. I called the National Influenza Centre and, within hours, a professional came to my home where she collected our samples donned in full personal protective equipment (PPE). This stood in stark contrast to when I’d travelled from New York to Kenya a month before. In the US, I struggled to obtain the necessary PCR test. When I did, my sample was taken by a nurse whose only protection from the hundreds of potential carriers she encountered each day was a surgical mask…When I flew to Kenya in late January 2020, for instance, airport officials had already implemented checks and contact tracing protocols. Even in March 2020, airports in Europe and the US were still largely operating as usual.
Political theorist Achille Mbembe has rightly criticized modernizing urban models that imagine and represent contemporary African cities only as the “sign of a lack,” invariably resulting in a scramble for the causes of, and solutions to, that lack.[43] As a result, we know more about what African cities are not than what they actually are. In keeping with this essay’s core aim to overturn commonplace readings of urban Africa, this section foregrounds local responses to COVID-19 in African cities, with an emphasis on the vital role of governance over government; that is, the hybrid arena in which formal and informal actors interact to make decisions.
For most African cities and governments, early preparation was the best preventative measure against COVID-19. This section’s opening quote describes the effective mitigation plans established by African city governments and local communities in response to the COVID-19 outbreak. Meanwhile, the individualistic cultures of the Western world were preoccupied with the lawfulness of enforced social distancing and politicized the wearing of face masks. Many cities across Europe and North America have seen anti-mask movements involving thousands of protesters. In contrast, an August 2020 poll by the Partnership for Evidence-based COVID-19 Response found that over 85 percent of respondents in 18 African countries said they had worn a face mask in the previous week.[44] Africa’s proactive and collectivist response to the COVID-19 pandemic merits more sustained and systematic analysis. According to the former Rwandan health minister Agnes Binagwaho, “COVID-19 has shown that the Western world and the Global North are not the best at doing everything. It’s time to revisit why they’re doing what they’re doing. The culture of individualism, the lack of solidarity—it’s losing trust with the people. And it’s making people sick.”[45] Binagwaho’s claim finds support in a recent study that concludes that people in collectivistic regions are more likely to wear masks than people in individualistic regions. In the former, the authors argue, people consider mask-wearing not only a duty, but also a symbol of solidarity—of joining hands to fight the deadly pandemic.[46]
Early aggressive and networked actions taken by African Union member states, spearheaded by city governments and civil society bodies, also staved off exponential transmission of the virus and saved lives. Africa CDC activated its Emergency Operations Center for COVID-19 on January 27, 2020, and the first COVID-19 meeting of African health ministers was held the following month, weeks before the continent detected its first case.[47] Once detected, a three-pillared COVID-19 Joint Continental Strategy was developed by Africa CDC that prioritized preventing COVID-19 transmission, deaths, and socio-economic harm.[48] At least 26 African countries took immediate and radical steps to curb transmission rates by instituting full or partial lockdowns; closing borders, churches, and mosques; requiring face coverings in public spaces; limiting domestic and international travel, including suspending direct flights to and from China; and establishing contact tracing and isolation practices. By way of an illustration, as early as January 2, 2020, Côte d’Ivoire started screening all passengers who had recently travelled to China. Given the urban bias of the virus and the socially-networked nature of urban Africa, cities emerged as the cutting edge of national prevention strategy. Public health protocols in congested urban settings included intense social distancing measures, prohibiting large gatherings at funerals and parties, shutting down places of worship and learning, cutting back on the common practice of overcrowded public transportation services, and strictly enforcing dusk-to-dawn curfews. Many urban authorities in Africa were active on social media, providing consistent and clear public health measures and sound scientific guidelines meant to keep citizens safe.[49]
In the Nigerian city of Port Harcourt, the government introduced a law in June 2020 that limited the number of funeral attendees to 50 and mandated that all public burials be approved by the state governor.[50] Even when officials relaxed restrictions on public transport, they made face masks compulsory and limited passenger numbers to allow for more physical distance between people. In Lagos, there was often an employee standing in front of the bus rapid transits dispensing sanitizer onto passengers’ hands. In Nairobi, volunteers from the Sonko Rescue Team (SRT), a rapid response NGO funded by Governor Mike Sonko, played a vital role in curbing the spread of COVID-19 in the capital city by working with the government to fumigate streets, distribute basic items to thousands of families in Nairobi’s informal settlements, and install sanitation booths in public spaces across the city. Churches and mosques in Nairobi also benefitted from SRT’s donations, including water tanks, hand washers and sanitizers, face masks, and automatic digital thermo guns.[51]
Across African cities, billboards, banners, vehicle slogans, and wall graffiti urged city-dwellers to wear face masks, wash their hands, and social distance (Fig. 2). Urban governments invested in mask production and adopted a zero-tolerance approach to going maskless in public spaces. Public compliance with restrictions was generally high, despite the centrality of movement to survival in African cities. Africa CDC Director Nkengasong has argued that the coordinated and aggressive reactions to the COVID-19 outbreak by African cities and governments explain the lower-than-expected impact of the pandemic on the continent: “Countries were shutting down and declaring states of emergency when no or single cases were reported. We have evidence to show that that helped a lot.”[52]
Figure 2: A COVID-19 banner in the city of Kano, Nigeria [53]
A prime example is Rwanda, which reported its first COVID-19 case on March 14, 2020 in a traveler who arrived in the capital city of Kigali. Within a week, commercial flights in and out of the landlocked country were halted, and from March 21 to April 30, the country instituted a full lockdown to limit intra- and intercity travel and strictly enforced mask use and social distancing of at least 1 meter. In this way, Rwanda was able to reduce local spread and ease the arduous process of contact tracing and isolation. Businesses that provided essential services like food, medicine, and fuel were permitted to remain open. Handwashing stations were mounted at many bus terminals. All inbound travelers were required to complete a 14-day quarantine at designated transit hotels and sites near their point of entry; they underwent screening for symptoms and were texted their results within eight to 24 hours. Those with mild symptoms were permitted to isolate at home by adhering to the government’s home-based COVID-19 management protocol, including daily contact with official health providers.[54] During the full lockdown, food and health-related palliatives were delivered to vulnerable households in recognition of the terrible toll of the pandemic. In addition to using robots to screen and monitor patients and locally-assembled drone technology to sensitize urbanites to the threats of the COVID-19 through public broadcasts, authorities in Kigali invested in digital money transactions and online shopping to reduce social interactions, especially in-person monetary exchanges.[55] Most of Rwanda’s COVID-19 testing took place in Kigali, where three of the four main public laboratories were located. By the end of April 2020, Rwandan health workers had tested more than 20,000 people.[56] In the ten months after its first case, Rwanda recorded only 133 COVID-19 related deaths, translating to a case fatality rate of 1.3 percent.[57] As of March 2022, the country had 129,601 cases and 1,459 deaths.[58]
Senegal is another African country whose pandemic response is exemplified by the proverb: “A stich in time saves nine.” Shortly after as the country confirmed its first case on March 2, 2020, President Macky Sall swiftly imposed curfews, bans on mass gatherings, temporary school closures, and travel restrictions between the country’s 14 regions. Despite having an under-resourced health system, Senegal ramped up COVID-19 testing capacity by operationalizing a cost-effective mobile lab system that had the capacity to return test results within a day.[59] As early as February 2020, Senegal’s Institut Pasteur de Dakar, a biomedical research center located in the capital Dakar, was one of just two laboratories in Africa that were able to test for COVID-19. The institute helped train staff from dozens of other African cities on testing, reinforcing the role of African cities as archives of knowledge.[60] Not surprisingly, Senegal was ranked second out of 36 countries on Foreign Policy’s COVID-19 Global Response Index, which provides a country-by-country assessment of government responses to the pandemic.[61]
At the same time that the securitization of pandemic responses in African cities may well have slowed the rate of COVID-19 transmission, it also came at hefty socioeconomic and human rights costs, especially for the many urban residents who could not afford the luxury of staying at home or remaining idle.[62] COVID-related space and time restrictions were enforced by law enforcement agents, who violently cracked down on urban residents who flouted lockdown curfews. In some countries, such as Uganda and Nigeria, governments utilized the pandemic as a justification for deploying scorched-earth tactics to quell peaceful urban protests against state corruption, police force extortion, and state failure, as well as to evict undesirable segments of the informal workforce like transport workers as part of elite-driven modernizing visions of building “world-class” African cities.[63] In other countries, such as Zimbabwe, the police have used COVID-19 restrictions as a pretext for suppressing media freedom and arresting the government’s main political opponents. In Nigeria, the COVID-19 lockdown measure was sudden and aggressive. As travel writer Noo Saro-Wiwa reported from the city of Port Harcourt: “[the lockdown] was announced on a Sunday. Citizens were given until Tuesday… to leave their jobs, hunker down at home and figure out alternative sources of income. Soldiers flogged people who were caught walking in the streets. The state governor cruised around town with an armed entourage and personally arrested individuals.”[64] In like vein, Johannesburg’s informal housing residents found their embodied and spatial routines of survival criminalized.[65]
Some city dwellers in Africa have claimed that state security forces are deadlier than the COVID-19 pandemic. While enforcing virus-related rules, law enforcement agents have killed ten people in South Africa, 12 in Uganda, 20 in Kenya, and 18 in Nigeria.[66] Far from quelling popular discontents, these extrajudicial killings have fanned the flames of massive protests across African cities, eliciting even deadlier police crackdowns. The economic fallout from COVID-19 and the selective and brutal enforcement of lockdown measures have compelled disaffected urban Africans, especially youths, to turn their space of marginality into a space of resistance. The #EndSARS protests that erupted across Nigerian cities in October 2020 were not only the result of decades of the brutal and unaccountable policing that is a legacy of colonialism; they were also a reflection of the spirit of the times, marked by the intensification of physical and social immobility caused by the securitization of COVID-19 responses. As one respondent from the city of Kano recounted:
People aren’t going to work, and 80 percent of Nigerians earn their livelihood through what they earn on a daily basis either in menial jobs, trading or what have you. All families are at wits end except the well to do. To make matters worse, the palliatives from government are hopelessly a joke.[67]
Previous experience with confronting public health emergencies in Africa, such as Ebola, cholera, malaria, Lassa fever, tuberculosis, and polio, have taught urban governments that engaging local communities, trusted leaders, and faith-based groups is key to convincing people to follow precautionary measures.[68] In major African cities like Freetown, Monrovia, Conakry, Lagos, Kinshasa, and Juba, existing Ebola protocols and infrastructures were repurposed to contain the COVID-19 crisis. This included early screening of new arrivals to the country, deployment of rapid-response teams, and meticulous contact tracing and isolation measures. In Nigeria, members of the national polio vaccination and eradication program adapted their expertise to tackle COVID-19. In Lagos, community health workers were deployed by local governments to send consistent and timely messaging about regular hand washing and sanitizing, social distancing, and mask wearing, drawing on best practices from Nigeria’s Ebola outbreak of July to October, 2014. These public health workers and knowledge brokers proved effective in connecting service providers to local communities and helping people recognize the symptoms of COVID-19.[69] In so doing, they plugged yawning gaps in Lagos’s health care system and demonstrated how people themselves can serve as a sort of anti-virus infrastructure.[70]
In Senegal, community leaders and itinerant health agents located in the capital city of Dakar constituted the spine of the West African country’s bottom-up pandemic response. They went from street to street to explain COVID-19 prevention protocols in a culturally respectful manner, hand out face masks and hand sanitizers, and talk about the effects of the pandemic on local radio. Their critical interventions persuaded many city dwellers to take precautionary steps and saved lives. Novotel, an upscale hotel in Dakar, emerged as a key isolation site for locals exposed to COVID-19 with a combination of hotel staff and Red Cross volunteers providing health care services. “When we talk to the population and tell them to face this COVID, it’s the community who can do it,” said Abdoulaye Bousso, who directs Senegal’s Health Emergency Operation Center in Dakar. “It’s not the health system, it’s the community.” According to the chief of infectious disease service at Dakar’s University of Fann Hospital Center, the “chain of solidarity” in Senegal was key to flattening the curve: “The nation joined hands together. Religious leaders came to join the political decision-makers, and also, the community involved themselves in giving this response to COVID-19.”[71]
In Freetown and Monrovia, the capitals of Sierra Leone and Liberia, taking the time to incorporate community members into public sensitization campaigns and working through trusted local leaders and urban social networks—both lessons learned during the Ebola epidemic—ensured a strong response to COVID-19. Both countries and capital cities re-instated the hand washing stands that had been central to limiting the spread of Ebola. As of September 2021, Sierra Leone had 6,393 confirmed COVID-19 cases and 121 deaths, while Liberia posted 5,794 cases and 283 deaths.[72] In African cities like Accra, Dakar, Nairobi, and Abidjan, religious communities—Christian and Muslim alike—united with each other and state agencies to limit the spread and impact of COVID-19 through shutting down their often-crowded places of worship, investing in prayer and fasting, distributing food to communities in distress, providing health supplies to medical facilities, keeping churches and mosques closed, and urging members to comply with precautionary measures laid down by the state, such as mask wearing and hand washing.[73] An example is the Presbyterian Church of Ghana, which provided free daily lunches for medical staff working at three major COVID-19 health centers in the capital city, Accra. Another example is the Islamic NGO Darul Hadith, which throughout the pandemic has distributed essential food items to the less-privileged in Accra’s Muslim inner cities.[74] One of Nairobi’s oldest churches, Christ Is the Answer Ministries, ran television, radio, and online broadcasts to 200,000 parishioners on Sundays, educating them about how COVID-19 spreads and urging members to take steps to protect themselves and others.[75] In short, the pandemic reinforced the powerful role of religion as a space of solidarity, collective leadership, healing, and hope in Africa’s urban public sphere.
Thirdly, with a median age of 19 years old, Africa’s population is the youngest in the world and tends to have fewer comorbidities. We know that COVID-19 is deadlier in older populations; only 3 percent of urban Africans are over the age of 65, compared to 20.8 percent in Europe. An estimated 91 percent of COVID-19 infections in African cities are among people below 60 years old.[76] Could demography have played a role in Africa’s lower-than-expected mortality rates? Most likely, yes—but the irony is not lost here. Too often, Africa’s urban “youth bulge” is seen as a soft underbelly. In the wake of COVID-19, however, it appears to have transformed into a strength of so-called “weak” cities.
Toward a Balance of Stories
The renowned Nigerian writer Chinua Achebe once said that stories have the power to dispossess or confer strength, depending on who tells them. My aim in this essay has not been to explain away dire (and in many cases, pre-COVID-19) realities of mounting unemployment, rising informality, and data gaps facing African cities. To the contrary, my objective has been to reclaim what Achebe calls a “balance of stories” in the interrogation of the ongoing pandemic, thereby underscoring the African city as what geographer Garth Myers calls an “important loci of global processes or generators of urban stories worth telling and worth learning from.”[77] Problematizing narratives that treat urban Africa as either extreme or exceptional, or the urban as though it were inseparable from Western modernity, this essay cautions against static ways of seeing non-Western cities that assume the worst at all times. Debunking COVID-19 stories that rob African communities of any agency or capacity for action, the essay called for a new approach shaped by hope instead of fear, one that invites us to learn and care about what African cities are doing. The call here is to move beyond the default premise that “cities in Africa just don’t work” and, instead, to pay critical attention to hybrid and adaptive governance systems emerging across urban Africa.
Many African cities shut down their airports and instituted lockdown measures much earlier than was done in other parts of the world. Crucially, African cities benefitted from comprehensive infection control plans that were built as part of efforts to manage previous epidemics. Finally, Africa’s collectivist cultures, community-led solutions, and young population played a role in limiting the ravages of COVID-19. The strong response of African cities to the crisis brings home an important lesson: Boasting advanced health care systems and superior financial power are not in themselves sufficient for tackling public health emergencies. The solidarity, proactive leadership, and indomitable optimism of African societies may actually have put them in a better position to more efficiently confront and contain public health crises than the more individualistic and rights-conscious cultures of so-called modernized and “world class” Western societies.
As African states now turn their attention to securing enough vaccines to inoculate their teeming populations, they encounter a Herculean challenge of “vaccine apartheid,” where wealthier nations seem to favor an individualist approach to a problem that will not be curbed unless addressed on a global scale. Although COVID-19 vaccines were developed in record time, roughly 66 percent of the countries around the world—the Global South accounting for the vast majority—have yet to receive a single vaccine dose. By contrast, ten countries have received 75 percent of the global vaccine supply, revealing the real inequalities that exist between centers and margins. In point of fact, only about 1 percent of adults in Africa have been vaccinated.[78] The unfolding painful surges in COVID-19 cases in African cities like Nairobi, Addis Ababa, and Kinshasa are reminders that the pandemic situation remains fluid, and that despite its early and admirable steps, Africa is not out of the woods yet.[79]
Daniel E. Agbiboa is assistant professor of African and African American studies at Harvard University, member of the Institute for Advanced Study at Princeton, and fellow at the Woodrow Wilson International Center for Scholars. His research interests lie at intersection of state and nonstate forms of order, and of mobility and mobilization, in urban Africa. He is the author of several books, including They Eat Our Sweat: Transport Labor, Corruption, and Everyday Survival in Urban Nigeria (Oxford University Press) and Mobility, Mobilization and Counter/Insurgency: The Routes of Terror in an African Context (University of Michigan Press).
[i] A type of residential real estate in urban Nigeria, where a group of one- or two-room apartments have entrances facing each other along a walkway leading to the main entrance.
[ii] Even the urban poor in Africa frequently go into huge debt to ensure an elaborate funeral for their loved ones.
Notes
[1] UN-Habitat, “Covid-19 in African Cities: Impacts, Responses and Policies” (report, UN-Habitat, UNCDF, UCLG-Africa, UNECA, New York: 2020), https://unhabitat.org/sites/default/files/2020/06/covid-19_in_african_cities_impacts_responses_and_policies2.pdf.
[2] UN-Habitat.
[3] Cara Anna, “Africa Should ‘Prepare for the Worst’ with Virus, WHO Says,” Associated Press, March 18, 2020, https://www.wivb.com/news/world/south-africas-coronavirus-cases-nearly-double-in-2-days/.
[4] Aryn Baker, “Few Doctors, Fewer Ventilators: African Countries Fear they are Defenseless against Inevitable Spread of Coronavirus,” Time, April 7, 2020, https://time.com/5816299/coronavirus-africa-ventilators-doctors/.
[5] BBC News, “Coronavirus: Africa Could Be Next Epicenter, WHO Warns,” BBC News, April 17, 2020, https://www.bbc.com/news/world-africa-52323375.
[6] “Vulnerable Continent: Africa and the Coronavirus,” France24, February 28, 2020, https://www.france24.com/en/20200228-vulnerable-continent-africa-and-the-coronavirus.
[7] “COVID Map: Coronavirus Cases, Deaths, Vaccinations, by Country,” BBC News, March 14, 2022, https://www.bbc.com/news/world-51235105.
[8] Ebun L. Bamgboye, Jesutonfunmi A. Omiye, Oluwasegun J. Afolaranmi, Mogamat Razeen Davids, Elliot Korateng Tannor, Shoyab Wadee, Abdou Niang, Anthony Were, and Saraladevi Naicker, “COVID-19 Pandemic: Is Africa Different?” Journal of the National Medical Association 113, no. 3 (June 2021), 324–335.
[9] Comaroff and Comaroff; Jennifer Robinson, “The Urban Now: Theorizing Cities Beyond the New,” European Journal of Cultural Studies 16, no. 6 (2013), 659–677; James Ferguson, Myths and Meanings of Urban Life on the Zambian Copperbelt (Berkeley, California: California University Press, 1999).
[10] Stephanie Newell, Histories of Dirt: Media and Urban Life in Colonial and Postcolonial Lagos (Durham: Duke University Press, 2020).
[11] Daniel E. Agbiboa, “Conflict Analysis in ‘World Class’ Cities: Urban Renewal, Informal Transport Workers, and Legal Disputes in Lagos,” International Journal of Urban & Regional Research 29 (2018), 1–18.
[12] Mfaniseni F. Sihlongonyane, “The Global, the Local and the Hybrid in the Making of Johannesburg as a World Class African City,” Third World Quarterly 37, no. 9 (2016), 1607–1627.
[13] Comaroff and Comaroff, 114.
[14] Chinua Achebe, “Africa Is People,” The Massachusetts Review 40, no. 3 (1999), 313–321.
[15] AboudMaliq Simone, “People as Infrastructure: Intersecting Fragments in Johannesburg,” Public Culture 16, no. 3 (2004), 407–429.
[16] Matthew Gandy, “Learning from Lagos,” New Left Review 33 (2005), 37–53.
[17] Rem Koolhaas, Lagos: How It Works (Baden: Lars Muller Publishers, 2007).
[18] Comaroff and Comaroff, 116; Jennifer Robinson and Ananya Roy, “Debate on Global Urbanisms and the Nature of Urban Theory,” International Journal of Urban and Regional Research 40, no. 1 (2016), 181–186; Jennifer Robinson, Ordinary Cities: Between Modernity and Development(London: Routledge, 2006); Tim Edensor and Mark Jayne, eds., Urban Theory Beyond the West: A World of Cities (London: Routledge, 2012); Achille Mbembe and Sarah Nuttall, “Writing the World from an African Metropolis,” Public Culture 16, no. 3 (2004), 347–372.
[19] Joe Bavier, “At Least 300,000 Africans Expected to Die in Pandemic: U.N. Agency,” Reuters, April 17, 2020, https://www.reuters.com/article/us-health-coronavirus-africa-un/at-least-300000-africans-expected-to-die-in-pandemic-u-n-agency-idUSKBN21Z1LW.
[20] For example: Adam Taylor, “Africa may have been hit harder by covid-19 than anyone knew.” Washington Post, February 18, 2022. https://www.washingtonpost.com/world/2022/02/18/africa-covid-cases-number-study/
[21] Comaroff and Comaroff, 112.
[22] Allen Neil Gerlach, “From Outbreak to Pandemic Narrative: Reading Newspaper Coverage of the 2014 Ebola Epidemic,” Canadian Journal of Communications 41 (2016), 611–630.
[23] Andrew Harding, “Coronavirus in South Africa: Scientists explore surprise theory for low death rate,” BBC News, September 3, 2020, https://www.bbc.com/news/world-africa-53998374.
[24] Center for Infectious Disease Research and Policy, “India, Brazil Grapple with Massive COVID-19 Surges,” University of Minnesota, April 15, 2021, https://www.cidrap.umn.edu/news-perspective/2021/04/india-brazil-grapple-massive-covid-19-surges.
[25] Priscilla Wald, Contagious: Cultures, Carriers and the Outbreak Narrative (Durham: Duke University Press, 2008), 7; Gerlach.
[26] Catherine D’Andrea, Twitter post, September 2, 2020, 9:55 p.m., https://twitter.com/CathyDAndrea99/status/1301337955580211200.
[27] Raymond Mpubani, Twitter post, September 3, 2020,
https://twitter.com/gonza_3010/status/1301476202528604160?ref_src=twsrc%5Etfw.
[28] BBC News Africa, Twitter post, September 3, 2020, 1:50 p.m., https://twitter.com/BBCAfrica/status/1301578309160009731.
[29] “COVID Map: Coronavirus Cases, Deaths, Vaccinations, by Country,” BBC News, March 14, 2022, https://www.bbc.com/news/world-51235105.
[30] Adia Benton, “COVID-19 in Ebola’s Wake: Safe Haven in Sierra Leone?” Current History 120, no. 826 (2021), 169–70. Emphasis in original.
[31] Chris Smith, “Scientists Can’t Explain Puzzling Lack of Coronavirus Outbreaks in Africa,” New York Post, September 4, 2020,https://nypost.com/2020/09/04/scientists-cant-explain-puzzling-lack-of-coronavirus-outbreaks-in-africa/.
[32] Ruth Maclean, “A Continent Where the Dead are not Counted,” New York Times, January 2, 2021, https://www.nytimes.com/2021/01/02/world/africa/africa-coronavirus-deaths-underreporting.html.
[33] Carolyn Gallaher, The Politics of Staying Put: Condo Conversion and Tenant Right-to-buy in Washington, DC, (Philadelphia: Temple University Press, 2016), 48.
[34] Excess deaths is a measure that compares actual deaths over a period of time with the number of deaths expected based on the same period in previous years. See BBC News, “Measuring Africa’s Data Gap: The Cost of Not Counting the Dead,” BBC News, February 22, 2021, https://www.bbc.com/news/world-africa-55674139.
[35] BBC News, “Measuring Africa’s Data Gap.”
[36] Former Red Cross official, in discussion with the author, November 6, 2020.
[37] Maclean.
[38] “Coronavirus: Health Chief Hails Africa’s Fight against COVID-19,” BBC News, September 23, 2020, https://www.bbc.com/news/world-africa-54248507.
[39] Chimamanda Adichie, “The Danger of a Single Story,” October 7, 2009, TED video, https://www.ted.com/talks/chimamanda_ngozi_adichie_the_danger_of_a_single_story?language=en.
[40] Mbembe and Nuttall, 356.
[41] Mbembe and Nuttall, 351; Comaroff and Comaroff.
[42] Mamka Anyona, “Africans Don’t Just Live to Die: A Response to The New York Times,” African Arguments, January 8, 2021, https://africanarguments.org/2021/01/africans-dont-just-live-to-die-a-response-to-the-new-york-times/.
[43] Achille Mbembe, On the Postcolony: Studies on the History of Society and Culture (Berkeley: University of California Press, 2001), 8.
- [44] Aryn Baker, “Why Africa’s COVID-19 Outbreak Hasn’t Been as Bad as Everyone Feared,” Time, December 30, 2020, https://time.com/5919241/africa-covid-19-outbreak/.
[45] Eli M. Cahan, Eli, “Rwanda’s Secret Weapon against COVID-19: Trust,” The BMJ 371 (December 11, 2020),https://www.bmj.com/content/bmj/371/bmj.m4720.full.pdf.
[46] Jackson G. Lu, Peter Jin, and Alexander S. English, “Collectivism Predicts Mask Use During COVID-19,” Proceedings of the National Academy of Sciences of the United States 118, no. 23 (2021), 1–8.
[47] Marguerite Massinga Loembé, Akhona Tshangela, Stephanie J. Salyer, Jay K. Varma, Ahmed E. Ogwell Ouma, and John N. Nkengasong, “COVID-19 in Africa: The Spread and Response,” Nat Med 26 (2020), 999-1003.
[48] Thomas Tieku, “The African Union Makes its Mark in the Pandemic,” Current History 120, no. 826 (2021), 172–177; Amy S. Patterson and Emmanuel Balogun, “African Responses to COVID-19: The Reckoning of Agency?” African Studies Review 64, no. 1 (2021), 1–24.
[49] Patterson and Balogun.
[50] Noo Saro-Wiwa, “COVID-19 in Nigeria,” The Round Table 110, no. 1 (2021), 79.
[51] Michael Majanga, “Why Sonko Rescue Team was recognized in fight against COVID-19,” TV 47, October 17, 2020, https://tv47.co.ke/2020/10/17/why-sonko-rescue-team-was-recognised-in-fight-against-covid-19/.
[52] Jina Moore, “What African Nations are Teaching the West about Fighting the Coronavirus,” New Yorker, May 15, 2020, https://www.newyorker.com/news/news-desk/what-african-nations-are-teaching-the-west-about-fighting-the-coronavirus.
[53] Daniel E. Agbiboa, photograph, June 11, 2020, Kano, Nigeria.
[54] Clarisse Musanabaganwa et al., “One Hundred Thirty-Three Observed COVID-19 Deaths in 10 months: Unpacking Lower than Predicted Mortality in Rwanda,” BMJ Global Health 6 no. 2 (2021), https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7907833/pdf/bmjgh-2020–004547.pdf.
[55] Youssef Travaly and Aretha Mare, “Learning from the Best: Evaluating Africa’s COVID-19 Responses,” Brookings Institution, July 8, 2020, https://www.brookings.edu/blog/africa-in-focus/2020/07/08/learning-from-the-best-evaluating-africas-covid-19-responses/.
[56] Moore.
[57] Clarisse Musanabaganwa et al.
[58] “COVID Map: Coronavirus Cases, Deaths, Vaccinations, by Country,” BBC News, March 14, 2022, https://www.bbc.com/news/world-51235105.
[59] Deirdre Shesgreen, “Senegal’s Quiet COVID Success: Test Results in 24 Hours, Temperature Checks at Every Store, and No Fights Over Mask,” USA Today, September 6, 2020, https://www.usatoday.com/story/news/world/2020/09/06/covid-19-why-senegal-outpacing-us-tackling-pandemic/5659696002/.
[60] “Coronavirus in Senegal: Keeping COVID-19 at Bay,” BBC News, October 5, 2020, https://www.bbc.com/news/world-africa-54388340.
[61] “COVID-19 Global Response Index,” Foreign Policy, August 5, 2020, https://globalresponseindex.foreignpolicy.com/.
[62] Awino Okech, David Mwambari, and Funmi Olonisakin, “COVID-19 responses and human rights in selected African countries,” Australian Journal of Human Rights 26, no. 3 (2020), 549–555.
[63] Agbiboa, “Conflict Analysis in ‘World Class’ Cities.”
[64] Saro-Wiwa.
[65] Caroline Wanjiku Kihato, Sarah de Villiers, Sumayya Mohamed, and Bonolo Mohulatsi, “Spatial Injustice in Johannesburg in the Time of COVID-19,” Current History 120, no. 826 (2021), 178–182.
[66] Max Bearak and Rael Ombuor, “Police Killed at least 20 Kenyans while Enforcing Coronavirus Rules. Hopes for Justice are Fading,” Washington Post, December 20, 2020, https://www.washingtonpost.com/world/africa/coronavirus-kenya-police-shootings-curfew/2020/12/20/deb81d5a-3efc-11eb-b58b-1623f6267960_story.html; Alison Sargent, “Curfew Crackdowns in Several African Countries Kill More People than COVID-19,” France24, April 17, 2020, https://www.france24.com/en/20200417-papers-curfew-crackdowns-in-several-african-countries-kill-more-people-than-covid-19; “Uganda—Where Security Forces may be Deadly than Coronavirus,” BBC News, July 23, 2020, https://www.bbc.com/news/world-africa-53450850.
[67] Resident of Kano, in discussion with the author, November 6, 2020.
[68] RCCE Collective Service, “Finding Community-Led Solutions to COVID-19,” Risk Communication and Community Engagement Technical Working Groups in East and Southern and West and Central Africa, 2020, https://extranet.who.int/goarn/sites/default/files/Community_Led_Solutions_COVID-19_Africa_Interagency_Guidance%20Note_FINAL_03072020%20%28003%29.pdf.
[69] Evaborhene Aghogho Nelson, “Shifting Frontlines in West Africa: Leveraging Community Health Promoters to Protect Vulnerable Populations against Covid-19 and other threats in Nigeria,” Think Global Health, June 17, 2020, https://www.thinkglobalhealth.org/article/shifting-front-lines-west-africa.
[70] Simone.
[71] Jen Kirby, “How Senegal Stretched its Health Care System to Stop COVID-19,” Vox, April 28, 2021, https://www.vox.com/22397842/senegal-covid-19-pandemic-playbook.
[72] Johns Hopkins University, “Coronavirus Resource Center,” Johns Hopkins University, September 28, 2021, https://coronavirus.jhu.edu/region.
[73] WHO Africa, “Religious Leaders Join COVID-19 Fight in Africa,” WHO, April 23, 2020, https://www.afro.who.int/news/religious-leaders-join-covid-19-fight-africa.
[74] Charles Prempeh, “Religion and the State in an Episodic Moment of COVID-19 in Ghana,” Social Sciences & Humanities Open 4, no. 1 (2021), 1–18.
[75] WHO Africa.
[76] Bamgboye.
[77] Chinua Achebe, Home and Exile (New York: Oxford University Press, 2000); Garth Myers, African Cities: Alternative Visions of Urban Theory and Practice (London: Zed Books, 2011), 6.
[78] Ans Irfan, Christopher Jackson, and Ankita Arora, “We Must Enhance—But Also Decolonize—America’s Global Health Diplomacy,” Scientific American, April 5, 2021, https://www.scientificamerican.com/article/we-must-enhance-mdash-but-also-decolonize-mdash-americas-global-health-diplomacy/; Michelle Gavin, “Supporting African Vaccinations is in U.S. and Global Interests,” Council on Foreign Relations, April 29, 2021, https://www.cfr.org/blog/supporting-african-vaccinations-us-and-global-interest.
[79] Mohammed Yusuf, “Kenyan Authorities Worried by Rise in New COVID Infections,” VOA, March 23, 2021, https://www.voanews.com/covid-19-pandemic/kenyan-authorities-worried-rise-new-covid-infections; U.S. Embassy in Ethiopia, “COVID-19 Rates Spiking; Hospital Beds for COVID Patients Full,” March 24, 2021, https://et.usembassy.gov/health-alert-covid-19-rates-spiking-hospital-beds-for-covid-patients-full/; Peter Mwai, “Coronavirus in Africa: Concern Growing Over Third Wave of COVID-19 Infections,” BBC News, June 9, 2021, https://www.bbc.com/news/world-africa-53181555.